Audience: Legislators • Committee analysts • Medicaid agency staff • Journalists
The Problem
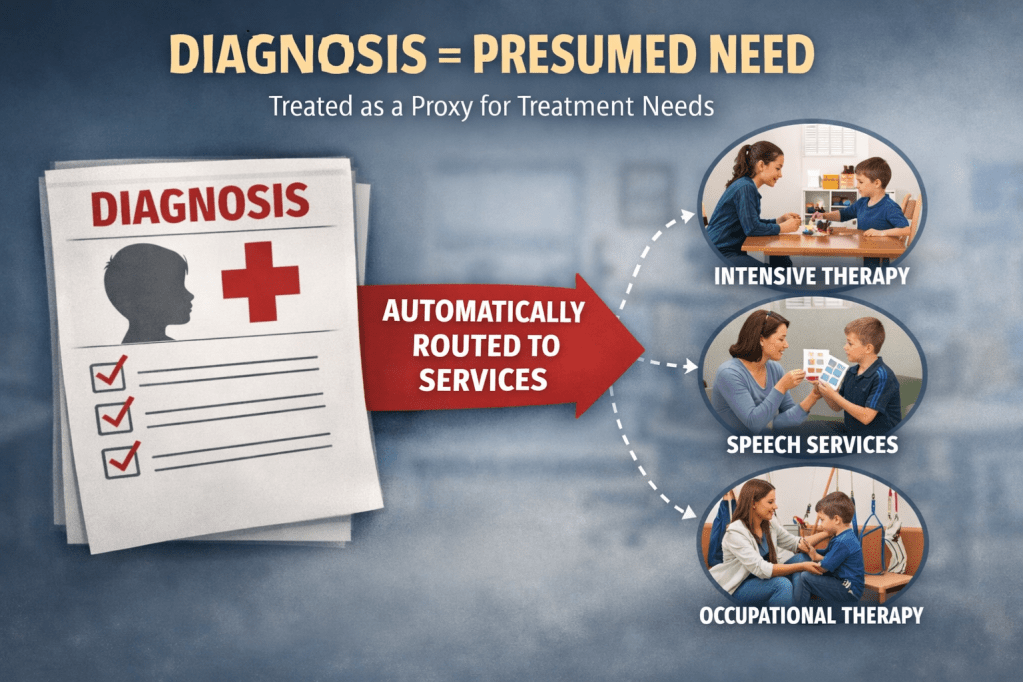
In many Medicaid and insurance policies, a diagnosis is treated as a proxy for treatment needs.
Once a diagnosis, particularly autism, is recorded, systems often assume impairment and route children automatically into intensive therapy programs. The result is a policy pathway that looks like this:
Diagnosis → Presumed Need → Automatic Service Pathways
This structure bypasses the central step used throughout healthcare: individualized evaluation of functional needs.
When diagnosis alone triggers services, programs risk:
- directing intensive therapy toward children who may not need it,
- overlooking the specific functional challenges that actually require treatment, and
- creating program structures based on diagnostic categories rather than clinical assessment.
Healthcare policy should ensure that treatment decisions follow documented needs and symptoms, not diagnostic labels.
In many Medicaid and insurance systems, a diagnosis is often treated as a proxy for treatment need—triggering automatic service pathways rather than individualized clinical evaluation.
Lawmakers who oversee federally matched programs carry a fundamental responsibility: identifying and interrupting the policy pipelines that allow waste, fraud, abuse, and neglect to persist within publicly funded systems. In Medicaid, where federal and state dollars are tightly intertwined, failures in oversight rarely remain local problems for long. They become matters of federal concern, triggering audits, clawbacks, and program scrutiny that can ripple across state systems.
Federal Clawbacks function as one of the United States Government’s most powerful deterrents. When improperly billed services are identified, individual states can be required to return federal matching funds, creating strong incentives for legislatures and agencies to examine how services are authorized, delivered, and reimbursed. Idaho’s decision this year to remove Applied Behavior Analysis (ABA) from its Medicaid billables illustrates the degree to which some states are already reacting to this pressure, seeking to limit exposure to federal audit risk before enforcement actions escalate.
Recent events in Minnesota demonstrate why such scrutiny is unlikely to fade. Large-scale fraud investigations there initially surfaced within an autism clinic, drawing federal attention to the broader structure of billing practices within programs involving children.
Centers for Medicare & Medicaid Services (CMS) reviews begin with a single cause of action. Once an audit is warranted, the CMS OIG evaluates whether claims across the program meet the standards of medical necessity, documentation, and clinical fidelity that federal law requires. For ABA services in particular, the central question becomes whether the therapy being billed reflects the intervention as it was designed and validated. As a result, audits in several states have identified billing irregularities and documentation deficiencies, raising broader concerns about program integrity.
State lawmakers therefore face a delicate balancing act. Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) mandate requires states to provide medically necessary services for eligible children, but the mandate establishes a federal floor rather than an unlimited ceiling. Legislators responsible for stewarding taxpayer dollars must determine how to meet that floor without creating open-ended entitlement structures that invite misuse.
At the same time, lawmakers must remain attentive to the legal boundaries surrounding service reductions. When states move too aggressively to cut reimbursement rates or restructure benefits, they may face litigation alleging unlawful denial of medically necessary care under Medicaid’s Early and Periodic Screening, Diagnostic, and Treatment (EPSDT) mandate. In North Carolina, parents and advocacy groups filed suit against the state Department of Health and Human Services after reimbursement changes affecting autism therapy services, arguing that the reductions limited access to treatment required under federal Medicaid law. Similar disputes have emerged in Arizona, where families challenged state decisions to reduce reimbursement rates for autism therapy providers, contending that the changes could restrict access to services for children enrolled in Medicaid.
The task, then, is not simply to cut spending, but to recalibrate programs so that they fund only the narrow band of services that demonstrably meet medical necessity standards under EPSDT.
In short, simply lowering reimbursement rates will not resolve structural program integrity risks; without reforms to evaluation, authorization, and documentation standards, states may still face EPSDT litigation from families, federal audits by CMS and the HHS Office of Inspector General, and potential clawbacks of federal matching funds for improperly authorized services.
Policymakers must examine whether therapies billed under Medicaid are being delivered as intended, whether documentation reflects real clinical need, and whether program structures incentivize appropriate care rather than volume-based billing. In practice, this means focusing less on diagnostic categories and more on the integrity of the services themselves. The objective is not to reduce services indiscriminately, but to ensure that publicly funded programs operate within the guardrails that federal law already establishes. When oversight succeeds, it protects not only public funds but also the credibility of the healthcare programs that vulnerable families depend on.
A Humane and Ethical Principle
Public programs should fund therapy based on functional impairment identified through evaluation, not diagnosis alone.
The appropriate clinical pathway is straightforward:
Evaluation ordered → Needs identified → Targeted treatment
Under this framework:
- A diagnosis triggers assessment, not automatic therapy authorization.
- Clinicians identify specific functional deficits (communication, motor skills, adaptive functioning, etc.).
- Treatment is targeted to the documented needs of the individual child.
This approach aligns therapy services with the same medical necessity standards used across healthcare.
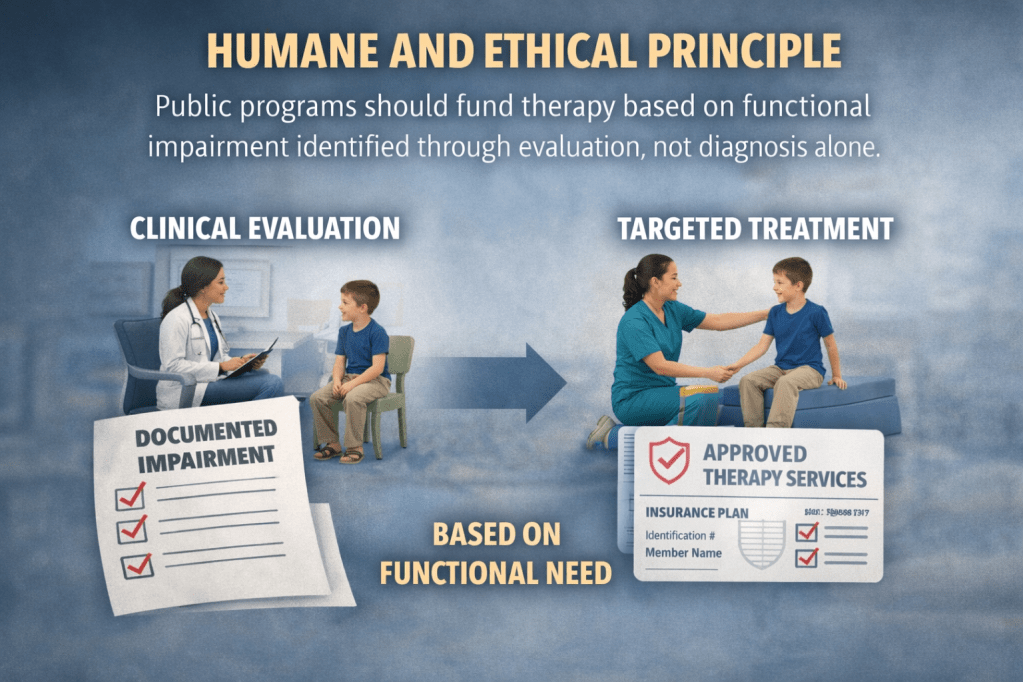
A humane and ethical approach to therapy funding prioritizes clinical evaluation and documented functional impairment, ensuring services are authorized based on individual needs—not diagnosis alone.
A humane and ethically grounded approach to publicly funded therapy begins with a simple clinical principle: services should be authorized based on demonstrated functional impairment identified through evaluation, not diagnosis alone. A diagnostic label can signal that further assessment is warranted, but it does not, by itself, establish the presence, severity, or nature of the challenges a child may be experiencing. Responsible healthcare policy therefore requires a step that is fundamental across medicine—an individualized evaluation that determines whether a specific functional limitation exists and whether therapy is likely to address it.
When treatment decisions are tied to documented needs rather than diagnostic categories, care becomes more precise and proportionate. Clinicians can identify the particular areas where support is necessary, communication, motor skills, adaptive functioning, or other domains, and design interventions that target those needs directly. Thus, liability shifts from lawmakers who inadvertently endorse regulatory gaps leading to fraud, and onto the allied health professionals who have specialized standards ingrained into their degree programs. This approach respects both clinical integrity and patient dignity by avoiding assumptions about what any diagnosis automatically entails.
Eligibility, Not Entitlement
In the United States, allied health clinicians must conduct an evaluation and document that a patient has a specific functional impairment, that therapy is medically necessary, and that there is a clear treatment plan with measurable goals. Having an autism diagnosis is not absolute evidence that any particular therapy is medically necessary.
For occupational therapy (OT), physical therapy (PT), speech-language pathology (SLP), and other rehabilitation services, a diagnosis alone does not automatically authorize treatment. Instead, services are approved when a clinical evaluation demonstrates functional impairment and medical necessity.
This is an eligibility-based model, not a diagnosis-based entitlement. Applying the same standard consistently ensures that public programs:
- support individualized care,
- maintain clinical integrity, and
- allocate resources where treatment is actually needed.
TRICARE REPORT – Lindsey
Outcome Measurement and Autism Therapy Oversight
The TRICARE Autism Care Demonstration (ACD) was launched in 2014 by the Defense Health Agency to consolidate earlier pilot programs that reimbursed Applied Behavior Analysis (ABA) therapy for military families. The purpose of the demonstration was not only to provide access to services but also to evaluate whether ABA meets TRICARE’s evidence standards for medical effectiveness and appropriate coverage as a permanent benefit.
The program currently covers ABA services for TRICARE beneficiaries diagnosed with autism spectrum disorder (ASD), but it operates under a demonstration framework precisely because the Department of Defense continues to evaluate questions about clinical outcomes, provider qualifications, and program administration.
A central issue identified in policy discussions, including those raised in oversight reviews referenced in the Lindsey TRICARE report discussions, is the challenge of establishing consistent and measurable treatment outcomes for ABA services. In federal healthcare programs, continued reimbursement generally depends on evidence that treatment produces measurable health benefits such as:
- improvement in functioning
- maintenance of essential skills
- prevention of clinical decline
Outcome measurement is therefore built into the TRICARE autism program. Providers participating in the ACD must submit standardized outcome measures before treatment authorization is renewed, allowing program administrators to track changes in behavior, development, and family functioning over time.
These outcome requirements reflect a broader policy principle within federal healthcare programs: coverage must be tied to demonstrable clinical benefit rather than diagnosis alone. Even though a diagnosis of autism establishes eligibility for evaluation and treatment planning, TRICARE policy emphasizes that services must remain clinically necessary and appropriate, meaning providers must document the expected health benefit of therapy.
The ongoing analysis of the Autism Care Demonstration, including research reviews conducted by independent expert committees, continues to examine whether current ABA delivery models reliably produce measurable improvements for beneficiaries and how the program should evolve in the future.
Non-measurable outcomes in Applied Behavior Analysis (ABA) is still an ongoing challenge in outcome measurement in the autism services industry. As ABA providers are not allied health professionals, coverage decisions must be tied to demonstrated need and expected clinical benefit, not simply to the presence of a diagnostic label. This eligibility-based model ensures that healthcare services are delivered when they are likely to improve functioning, maintain essential skills, or prevent further decline. In short, medically necessary services must prove through measurable outcomes that there is a health benefit to the prescribed therapy.
If therapy is advertised to be provided by non-clinicians, the pipeline must end at that point of recommendation. We must consider re-evaluating the structural pipeline through which autism diagnoses are converted into automatic therapy authorizations. By grounding authorization in documented impairment and medical necessity, allied health programs maintain a consistent standard across healthcare: services are provided because they are needed and clinically justified, not because a diagnosis alone confers an automatic entitlement to treatment.
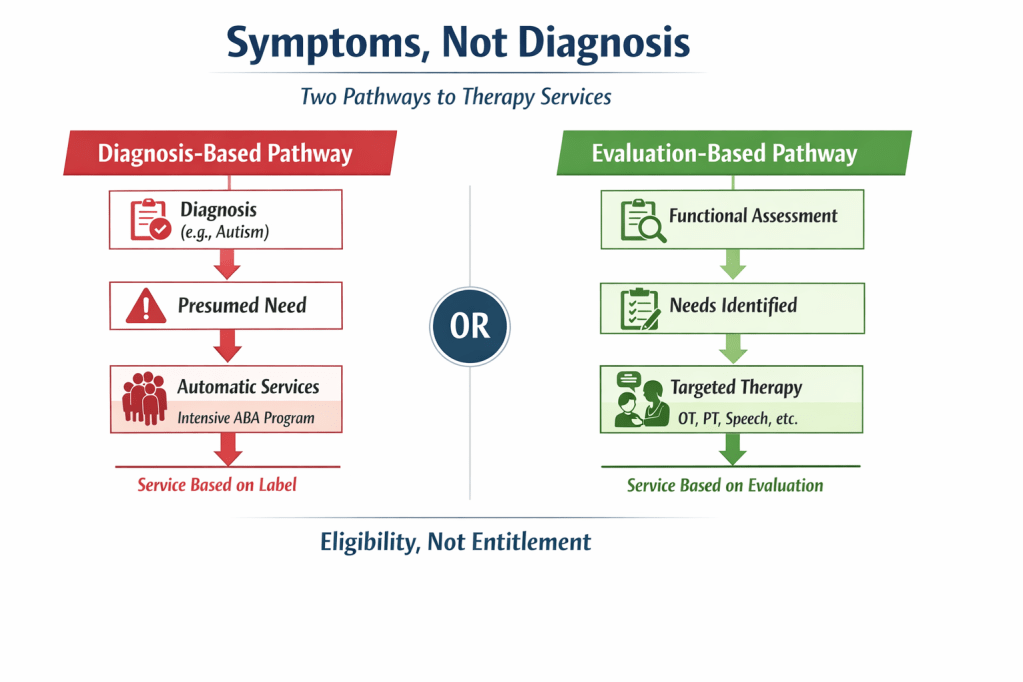
Virtual diagram showing two approaches to therapy access: diagnosis-based entitlement versus evaluation-based eligibility. Services should follow documented functional needs—> evaluation → identified needs → targeted treatment.
Lawmaker-Ready Takeaways
- A diagnosis should trigger evaluation—not guarantee therapy.
- Public programs should fund services tied to documented symptoms and functional needs.
- The appropriate pathway is evaluation → identified need → targeted treatment.
- Most therapy disciplines already operate on eligibility, not entitlement.
- Policies should ensure that treatment decisions follow clinical assessment, not diagnostic category.
- Aligning therapy with functional impairment helps deliver the right care for the right patient at the right time.
- This approach protects patients, clinicians, and public resources alike.

Leave a comment