What Autism Speaks Isn’t Saying About Congress’s 2026 Autism “Funding Win”
You’ve seen the headlines: Congress passes critical autism funding in Fiscal Year 2026 federal package: Autism Speaks helps ensure strong support for federal programs driving innovation, training and support for people with autism, February 10, 2026.
The 2026 federal autism funding package has been presented as a major policy victory, but the legislative record tells a quieter, more revealing story. There is no new agenda here, no structural reform, no shift in federal priorities. The decisive policy action occurred not in 2026 but in December 2024, when the Autism CARES Act was reauthorized, committing roughly $1.95 billion in federal spending through 2029 and reaffirming the architecture that has governed autism policy for years. By the time Congress passed the FY2026 appropriations bill, the contours of that system were already fixed. What lawmakers did was not to redesign it, but to keep it running. What is being framed as innovation is, in practice, continuity.
At the same time, a parallel messaging campaign centered on “profound autism” is emerging to reinforce that continuity. Figures within the Profound Autism Alliance, including Judith Ursitti, have centered claims that a small subset of autistic people, often cited as “6%”, require lifelong or 24/7 care. Claims often presented without consistent sourcing or clear methodological grounding are being used to generate urgency and justify expanded research and intervention systems.
Severity-based framing that prioritizes dependency and lifelong supervision aligns with intervention-focused service pipelines. Major advocacy organizations create a closed policy loop: autism severity framing drives funding, funding expands service markets, and those markets reinforce the original framing. The result is a self-sustaining system that prioritizes research and intervention infrastructure over autonomy, rights, and meaningful wellbeing outcomes. At the same time as aspects of the ABA sector face increasing federal scrutiny, including concerns around billing and program integrity, we offer this autistic-led exposé to unpack these messaging strategies and its fiscal impacts, now that budget hearings are in full swing.

Same System, New Headlines: What’s presented as a breakthrough is the continuation of an existing pipeline: repackaged, rebranded, and resold as progress.
December 23, 2024 — The Real Policy Decision Already Happened
To understand what is happening in 2026, it is necessary to return to 2024, when the Autism CARES Act quietly settled the question of federal direction for the remainder of the decade. The law did not introduce a new philosophy of autism policy so much as it reaffirmed an existing one, consolidating federal investment around research, surveillance, and professional training pipelines. These are not marginal programs; they are the core infrastructure through which autism is defined, measured, and acted upon at the national level. The National Institutes of Health continue to fund research agendas shaped by biomedical and behavioral frameworks. The Centers for Disease Control and Prevention expand surveillance systems that track prevalence and feed data back into those research pipelines. The Health Resources and Services Administration invests in training clinicians who operate within that same paradigm. Each component reinforces the others. Together, they form a stable system that does not require reinvention each fiscal year, only continued funding.
FY2026 Appropriations — Congress Simply Continued Existing Spending
This is the context in which the FY2026 appropriations bill must be read. Appropriations are often described in public-facing language as policy decisions, but in practice they are instruments of maintenance. They allocate resources to programs that have already been authorized, ensuring continuity rather than initiating change. The February 2026 announcement celebrating “critical autism funding” relies on a subtle conflation of these functions, presenting routine continuation as if it were legislative innovation. Contrary to Autism Speaks headlines, Congress did not debate whether to shift the center of gravity of autism policy toward housing, employment, or civil rights enforcement. It did not introduce new categories of support or meaningfully alter existing ones. It did not reconsider the balance between research investment and direct assistance. The bill simply ensured that the established system would continue to operate at scale.
The Research–Surveillance–Intervention Pipeline
Within that system, the emphasis on early identification and intervention remains largely unquestioned. Surveillance funding supports earlier and more comprehensive detection of autism across populations. Training programs expand the workforce capable of diagnosing and managing those cases. Research funding refines the models that justify and sustain intervention practices. The pipeline is not described explicitly in legislative language, but it is structurally embedded in how funds are distributed. By the time appropriations are made, the logic of the system is already assumed. What begins as identification moves seamlessly into intervention, and from there into long-term management. The system sustains itself not because each component is debated annually, but because the framework that binds them has already been accepted by the previous administration.
“Profound Autism” Descriptive Research Construct
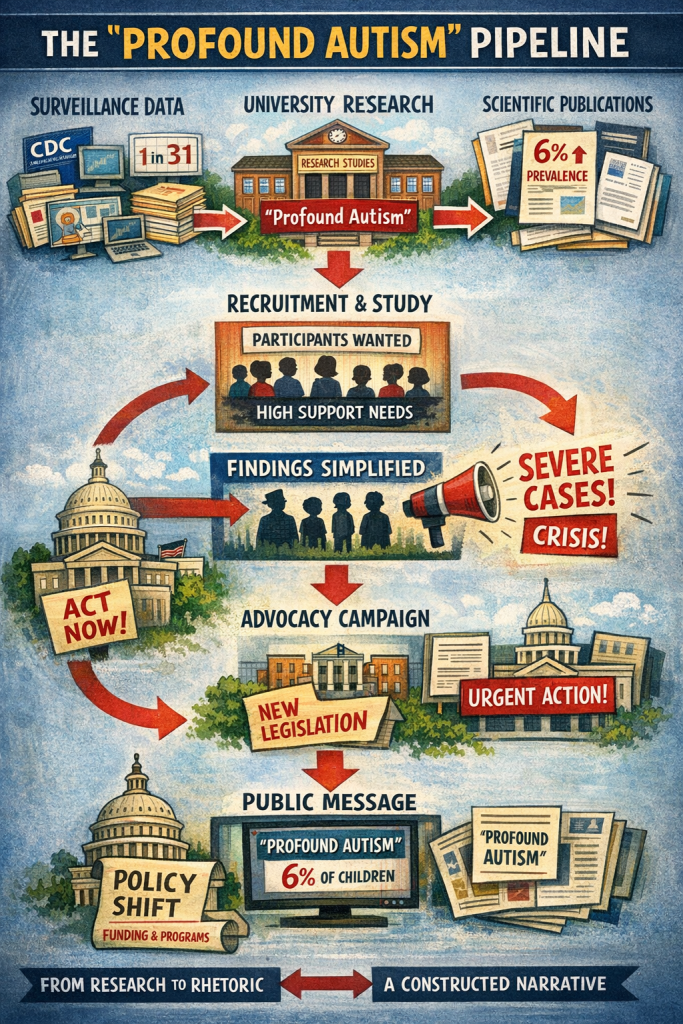
Beginning in 2000, the ADDM Network has been tracking the number and characteristics of 8-year-old children with ASD. The “profound autism” claim merely alleges a prevalence of subclassified people based on surveillance datasets through CDC ADDM reports. Meaning, if you want to imagine how many autistic people are at your child’s school, you would divide the current prevalence (1 in 31) by the number of children in the school–but that hardly constitutes a formal prevalence study. To promote a severity of needs entitlement in language that is comprehensible by lawmakers, stakeholders are increasingly channeling research through university-based programs.
The emergence of the “profound autism” narrative is not a discrete scientific development. Politically, it is a translation layer between unsettled research and policy that does not fully reflect the limitations of the underlying research. The strategic research pipeline becomes visible in the pathways through which ‘findings’ are operationalized and disseminated. As stakeholders frame severity in terms policymakers can understand, a shift is taking place in how these ideas are produced and presented. These constructs are increasingly embedded within public university research programs. There, institutional authority helps make these categories seem more defined and stable.
We have examined research activity within this emerging ‘profound autism’ framework. In Iowa, for example, principal investigators have circulated recruitment materials inviting caregivers to enroll children described as having been “diagnosed with Profound Autism.” Following public scrutiny, the university’s Institutional Review Board (IRB) indicated they revised the protocol to remove that phrasing from the recruitment material. Notwithstanding their defense, the Principal Investigator, expressed that the language is used for research purposes and not intended to be a scientific term.
The phrasing carries weight precisely because it bypasses the provisional nature of the medical science and presents it instead as an established diagnostic category. Recruitment, in this context, does not simply identify a population; it participates in creating one. As these research practices take hold, they begin to feed directly into advocacy narratives, where complexity is compressed into forms that can travel easily through policy discourse.
The frequently cited “6%” statistic functions as a rhetorical instrument. It signals urgency without providing a healthcare explanation. Profound researchers approximate higher-support subgroups using proxies such as intellectual disability and limited language. These analyses produce widely divergent estimates. They are often in the range of 20 to 30 percent or higher, depending on criteria.
A simple misreading of data is, in fact, a layered process in which research constructs, recruitment practices, and advocacy messaging converge and reinforce one another. By the time it reaches the level of federal discourse, it carries the authority of something already settled, even as the underlying definitions remain in flux. In this movement, the distinction between describing a population and constructing one becomes increasingly difficult to maintain, and the resulting narrative of a clearly bounded subgroup defined by severity and need, appears far more stable than the evidentiary base from which it emerged.
This analysis does not dispute that some autistic individuals have very high support needs; it examines how those needs are defined, quantified, and translated into policy.
When a Category Becomes Policy: What begins as a provisional research label is operationalized, amplified, and institutionalized, until it functions as settled truth in funding and legislation.
Provider Alignment and the CASP Signal
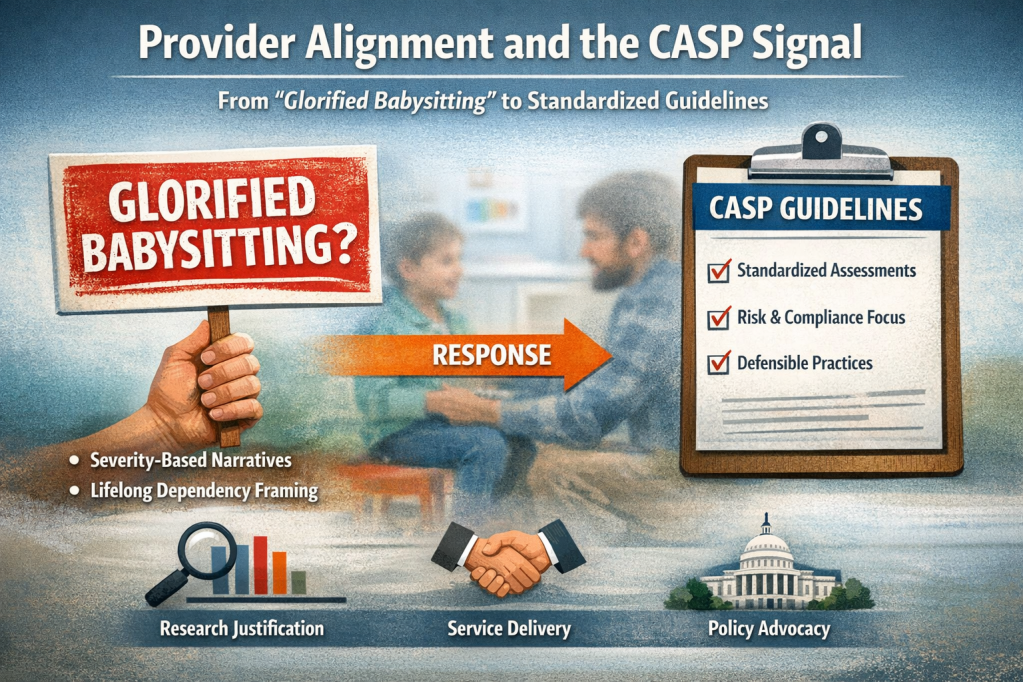
As severity-based narratives gain traction, they align with the institutional interests of service providers and the broader intervention ecosystem. The more autism is framed in terms of lifelong dependency and high support needs, the more those systems appear not only justified but indispensable. Provider organizations, particularly those operating within intensive behavioral intervention models, occupy a central position in this landscape. Their standards, guidelines, and public responses increasingly reflect a sector that is both expanding and defending its role within a scrutinized environment. When those positions are amplified or validated by large advocacy organizations, the boundaries between research justification, service delivery, and policy advocacy begin to blur.
This alignment becomes especially visible in the positioning of the Council of Autism Service Providers (CASP), whose assessment guidelines are now being elevated within the same policy environment. CASP has publicly rejected the characterization of ABA services as “glorified babysitting“.
The emergence of new, highly structured guidelines invites a different reading. In healthcare, guidelines typically appear when variability, risk, or liability requires formal containment. They are written not simply to improve care, but to define defensible boundaries of practice. Read in that light, the CASP guidelines function less as a breakthrough in clinical clarity and more as a document of system stabilization. They are codifying how services should be justified, documented, and delivered in an increasingly scrutinized landscape. The tone is clinical, but the subtext is risk management. The irony is difficult to miss: in responding to criticism, the field has produced a framework that quietly acknowledges the very pressures it seeks to dismiss.
From Critique to Compliance: As scrutiny grows, provider systems don’t shrink; they standardize, formalize, and align with policy, reinforcing the same intervention pipeline they are asked to justify.
The Policy Feedback Loop
What results is a feedback loop that is difficult to interrupt from within. Severity-based framing generates urgency. Urgency legitimizes funding. Funding expands systems that, in turn, produce data and institutional momentum reinforcing the original framing. Advocacy messaging consolidates these elements into a coherent narrative of progress, and policymakers respond by continuing to fund the system that has been presented to them. Within this loop, alternative priorities, autonomy, community-based supports, protections against coercion, remain structurally marginal.

The Policy Feedback Loop Behind “Profound Autism”: A closed system in which severity-based claims drive urgency, justify research funding, expand intervention markets, and reinforce advocacy narratives, ultimately shaping federal policy that sustains the same pipeline.
The $400 Million Narrative
The widely cited figure, “nearly $400 million” of alleged autism funding, is rhetorically powerful but structurally misleading. That funding flows through long-standing channels: NIH research, CDC surveillance, HRSA training programs, and a modest restoration of $8 million in Department of Defense autism research funding. None of these programs are new. All are embedded in the CARES Act ecosystem. Direct material support for families and children represents only a limited portion of this funding landscape, and is not the primary focus of these allocations.
With authorization secured through September 2029, federal autism policy is operating within a fixed cycle. Annual appropriations adjust funding levels but do not alter the underlying framework. The 2026 budget did not reopen debate. It funded the system already in place, one that continues to prioritize research and institutional infrastructure over direct, day-to-day support for families and children.
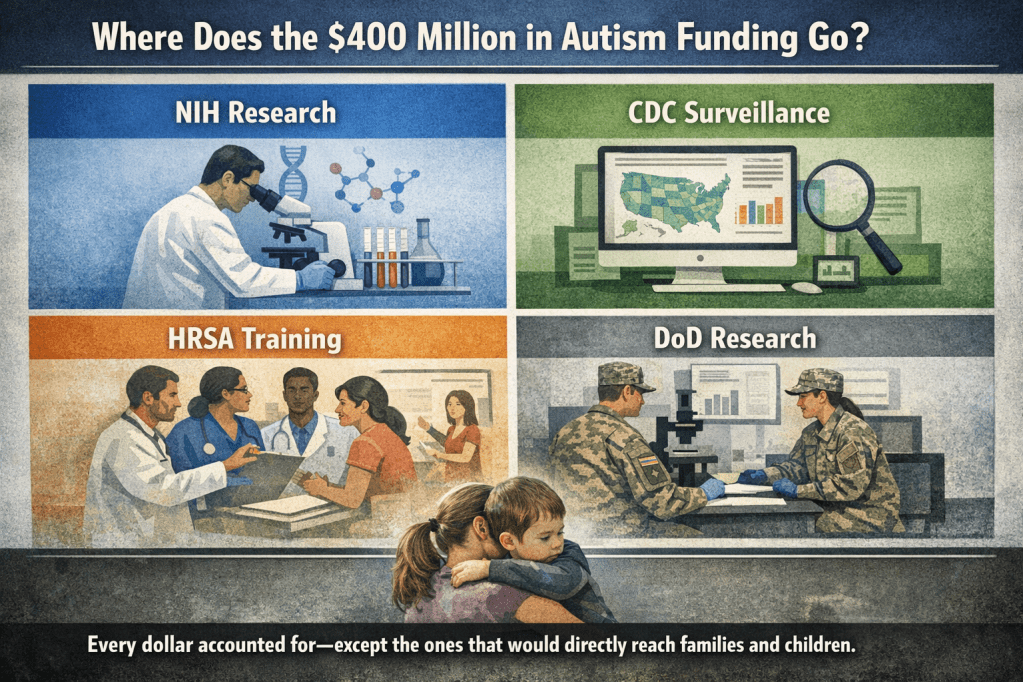
Where the $400 Million Goes and Where It Doesn’t: Federal autism funding sustains research, surveillance, and provider pipelines, while direct support for families and children remains structurally absent.
The Parallel Messaging Strategy
At the same time, a coordinated messaging shift is emerging. Within the “profound autism” advocacy space, claims that roughly six percent of autistic people require lifelong or 24/7 care are being deployed to generate urgency. These claims are rarely accompanied by transparent sourcing or consistent definitions, yet they function effectively as policy levers. By foregrounding severity, they justify continued investment in research and intensive intervention systems.
This narrative aligns with the interests of provider organizations whose business models depend on those systems. The convergence is not accidental. It reflects a shared incentive structure in which severity framing supports both funding and service expansion.
Taken together, these elements form a closed loop. Severity-based claims generate urgency. Urgency justifies research funding. Funding expands intervention systems. Provider organizations formalize and defend those systems. Advocacy groups amplify the narrative. Policymakers continue funding the same structure. The cycle repeats.
Within this loop, families and children are directly affected. Support is often mediated through the same intervention systems rather than delivered as flexible, community-based assistance. Resources are structured around programs and providers, not around the lived needs of families navigating daily care, communication, and long-term stability. As a result, autonomy, rights, and practical support remain peripheral, not because they lack importance, but because they are not embedded in the same institutional machinery.
Bursting the Bubble
If there is a bubble in federal autism policy, it is the belief that sustaining the same system year after year constitutes meaningful change. Bursting that bubble requires naming the difference between maintaining a structure and transforming it, and recognizing that, in 2026, the structure remains firmly intact.


Leave a comment