Many parents are told that things like aggression, anxiety, or “acting out” are just part of autism. But a recent study suggests something important: that’s often not the full picture.
Researchers in Germany looked at school-aged autistic children with average intelligence and used a screening tool called the Child Behavior Checklist (CBCL). This checklist helps identify patterns in areas like anxiety/depression, attention, social difficulties, aggression, rule-breaking, and more.
Read the study (free, open-access): Linnenbank, F., Linnenbank, M., Beimdiek, S., Bender, S., & Vöckel, J. (2026). Co-occurring Psychiatric Symptoms in Verbal, School-Aged Children With Autism Spectrum Disorder and at Least Average IQ. Journal of Autism and Developmental Disorders, 1-17.
What they found matters. These challenges showed up at much higher rates than in other children—and importantly, they were not strongly tied to how “severe” the child’s autism was. In other words, these are not simply autism traits. They may reflect separate, co-occurring mental health conditions.
That distinction is critical. Behaviors like aggression, emotional distress, or attention struggles are not part of the DSM-5 criteria for autism. When we assume “this is just autism,” we risk overlooking treatable mental health needs.
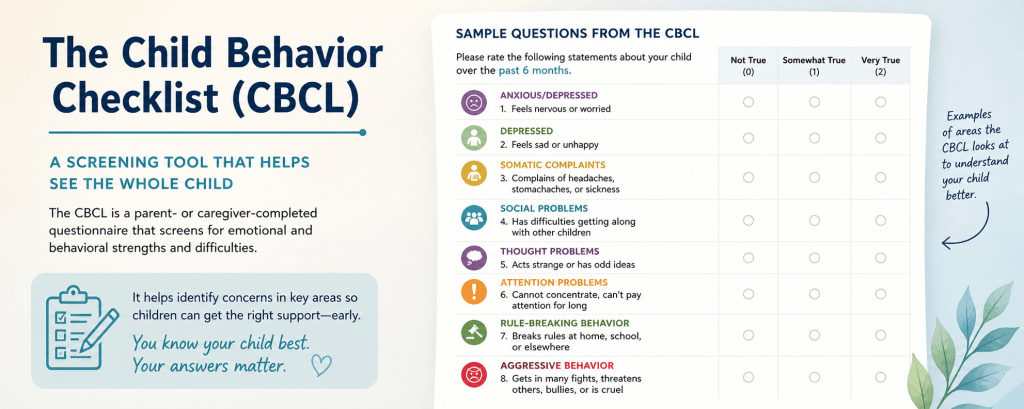
The CBCL is a straightforward screener that parents and clinicians can use together. It doesn’t diagnose—but it can help flag whether a deeper mental health evaluation is warranted. It looks at:
Aggression, anxiety/depression, somatic complaints, social problems, thought problems, attention problems, and rule-breaking behavior.
If your child is struggling in these areas, it’s reasonable to ask: Could this be something more than autism?
This also raises an important point about intervention. Behavioral approaches like ABA are often presented as the default response to “problem behaviors.” But ABA is not a mental health treatment. If a child is experiencing anxiety, depression, or emotional distress, those need to be understood and addressed directly.
Parents deserve better explanations than “this is just the autism.” Tools like the CBCL offer a starting point for asking more precise questions—and getting more appropriate support.
#Autism #MentalHealth #ParentAdvocacy #CBCL #Neurodevelopment #ChildPsychology
Resources:
The American Psychological Association (APA) recognizes the Child Behavior Checklist (CBCL) as a standardized, empirically validated tool for assessing behavioral and emotional problems in children. Completed by parents or caregivers, it includes over 100 items covering internalizing behaviors (e.g., anxiety, shyness) and externalizing behaviors (e.g., aggression, antisocial behavior). The CBCL is widely used to help identify patterns that may indicate the need for further mental health evaluation.
If you’re noticing behaviors in your child that don’t seem to match what teachers are reporting—or if you’re being told that aggression or “problem behaviors” are simply part of autism—it’s reasonable to ask for a more structured evaluation.
You can specifically request that your clinician use a standardized screener like the Child Behavior Checklist (CBCL). This helps move the conversation from subjective impressions (“this is just autism”) to a more systematic assessment of emotional and behavioral patterns, including anxiety, mood, and attention-related concerns.
It’s also appropriate to ask for a multi-informant approach, meaning input from both home and school is considered. Differences between parent and teacher reports are not unusual—they often reveal important context about when and where a child is struggling.
If behavioral interventions like ABA are being recommended based solely on aggression or distress, you can ask a clarifying question:
“Has my child been screened for co-occurring mental health conditions that could explain these behaviors?”
That question reframes the issue. It signals that behavior should be understood before it is treated, and that not all distress or aggression should be attributed to autism without further evaluation.
You’re not pushing back—you’re asking for a more complete clinical picture.
Read the study (free, open-access): Linnenbank, F., Linnenbank, M., Beimdiek, S., Bender, S., & Vöckel, J. (2026). Co-occurring Psychiatric Symptoms in Verbal, School-Aged Children With Autism Spectrum Disorder and at Least Average IQ. Journal of Autism and Developmental Disorders, 1-17.

Leave a comment